With the introduction of clear aligners, the demand for dental aesthetics is increasing and Global Invisible Orthodontics Sales Market Report (360 Research Reports, October 2020) shows the clear aligner market projected to grow at a rate of 11.5% each year.
Over the past few years, clear aligners have become very popular. Aligners are marketed as more aesthetic, comfortable, effective, and faster alternative to traditional braces.
However, are all clear aligners created equal? What should you, as the clinician, look for when offering clear aligners to your patients? Furthermore, what are some of the possible side effects caused by clear aligner treatment?
What are Some Characteristics of Clear Aligners?
The principal idea behind the function of clear aligners is similar to traditional braces; teeth are slowly moved and aligned over the treatment period. Clear aligners satisfy the demand for faster and more aesthetic treatment and are also prone to rapid technological improvements in aligner materials and production techniques.
The thermoplastic materials used, the gingival margin design, and the different strategies used to guide orthodontic movement such as attachments, divots, and auxiliary tools, converge in determining the effectiveness of a system of aligners.10 Clear aligners are not all the same, and consistent differences can be observed between different brands. Clinical indications for use were initially limited to the leveling and alignment of the arches in the presence of slight crowding or diastemas.13-14 Currently, aligners are also being used for correction of misalignments like rotated, crowded, or blocked-out teeth, open bite, cross bite, deep bite, edge-to-edge bite, overjet, teeth spacing, diastemas, midline shift, Curve of Spee, rotations, distalization and mesialization of posterior teeth accurately and discreetly.
Aligners are produced in various thickness levels ranging from 0.020 – 0.030 inch. They work by creating mild pressure on teeth and slowly push the teeth into the desired position. The use of gradually thickening aligners provides more control on tooth movement and reduces the pain caused by orthodontic forces, however, the same biomechanical principles apply.
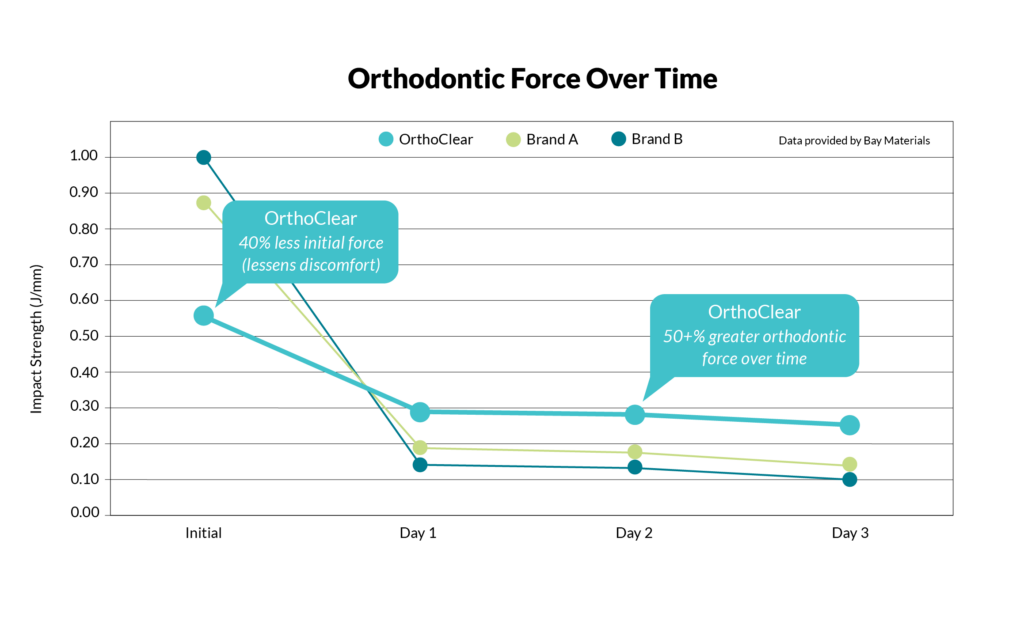
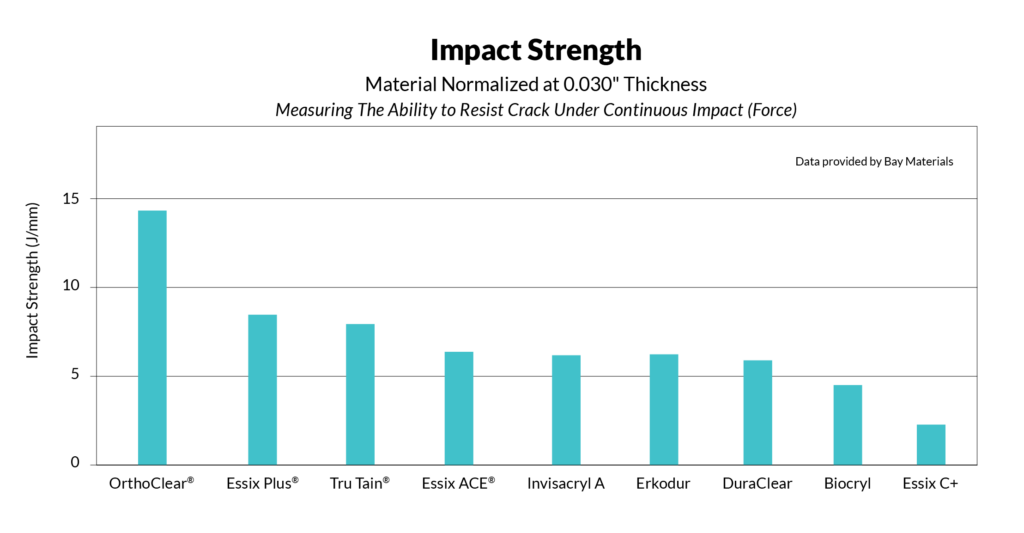
The aligners should provide gentle initial force for reduced pain, but continuous force to facilitate tooth movement. When it comes to clear aligners, choosing a premium material designed to optimize patient comfort and accurate tooth movement is crucial. Aligners made from a 0.76mm (0.03 inch) high-quality, stain and crack resistant multi-layer polyurethane has a tough polymer backbone, and a reputation as the benchmark for crack resistance. Cracking can occur when the patient removes the appliance. Long-term crack resistance and reduced breakage prevent unnecessary office visits and replacements, which lower costs for impressions and refits.
OrthoClear® aligners exhibit exceptional crack resistance characteristics when compared to aligners made from various other materials.

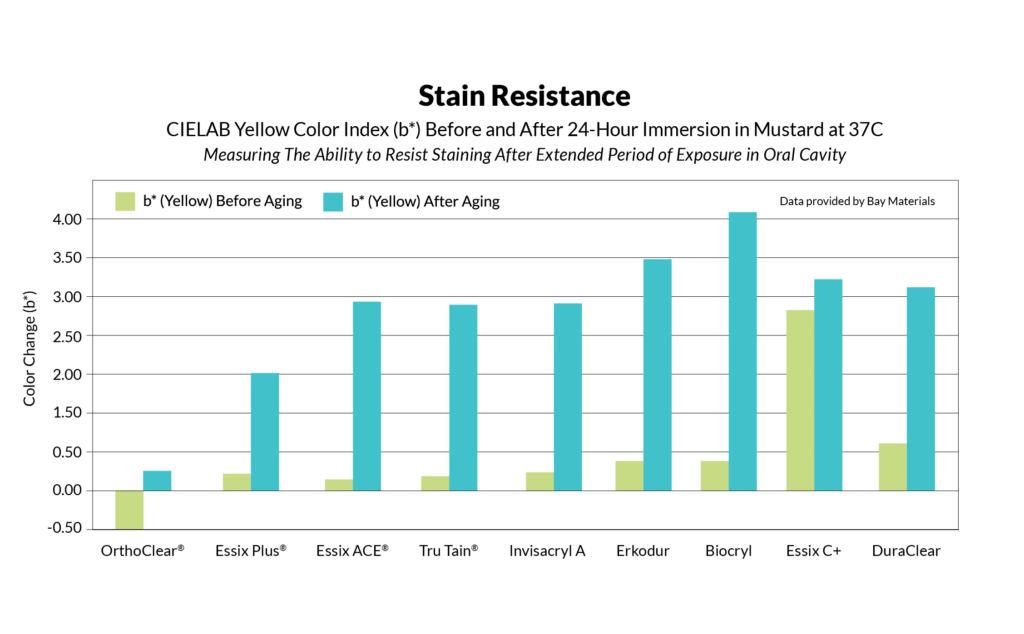
Clear aligners are susceptible to discoloration in contact with liquids and can lose their clarity over time. As a rule of thumb, it is best to avoid drinks that have a pH below 7.0.
Flavored water, energy drinks, fruit juices, drinks containing soda, or highly sugary or acidic drinks are some drinks that should be completely avoided. These liquids can easily penetrate through aligners and stay on the surface for a longer period, which can lead to discoloration of aligners and teeth.
Higher standards of aesthetics and unsurpassed clarity lead to improved patient compliance (and satisfaction). Greater patient satisfaction leads to higher referral rates.
Are There Any Adverse Effects of Clear Aligners?
Clear aligners are made of thermoplastic materials. The most commonly used materials are polyurethane, polyester, and polyethylene glycol terephthalate (PETG). The common chemicals BPA and phthalates have side effects from exposure that can have lifelong consequences. Phthalates and bisphenol A (BPA) are man-made chemicals that are known endocrine disruptors. They can affect hormones such as estrogen and testosterone, and potentially disrupt normal growth and development. It’s essential to choose an aligner material that’s BPA and phthalate free.
OrthoClear® aligners are a safer choice as they do not contain BPA or phthalates.
Several studies have been conducted over the past few years to assess the adverse effects of aligners on oral health. Breathing difficulty, sore throat and tongue, itchiness and hives, severe hypersensitivity reactions, and swelling in the lips are some side effects. At times wearing aligners may cause nausea, painful ingestion of food, dryness of mouth, and headaches. Rarely swelling of eyes and other concerns, like pain in the chest and cough, were also reported.
What’s Next After Clear Aligner Treatment?
As the number of adults treated with clear aligners increases, use of clear aligners facilitates oral hygiene, thus improving the periodontal status and causing a decrease in plaque levels, gingival inflammation, bleeding upon probing, and pocket depth.2, 40 Fixed appliances and wires can make plaque control difficult and have adverse effects on periodontal tissues, making orthodontic treatment a predisposing factor for periodontal diseases.43 However, according to the study by Han et al.40, with careful oral hygiene education and repeated plaque control, patients treated with fixed appliances and clear aligners showed similar gingival and plaque indexes.
Clear aligners not only promote better oral hygiene and better periodontal health, but also reduce plaque accumulation and the development of white spot lesions.
According to the study by Azeem et al.44, orthodontic treatment with clear aligners showed a low incidence of newly developed white spot lesions. Periodontitis etiology involves host inflammation triggered by the buildup of bacterial plaque biofilm.
This inflammation leads to subsequent loss of periodontal ligament, cementum, and alveolar bone, the attachment apparatus of the tooth. The use of PerioRestore® (DenMat, Lompoc, CA) or similar systems that contain 1.7% hydrogen peroxide gel, breaks up biofilm, kills bacteria, and keeps bacteria from recolonizing preventing further infection.
It would be a good idea to complete the treatment with a periodontal homecare system consisting of customized trays designed to gently push a 1.7% hydrogen peroxide gel deep into the periodontal pocket. According to a study by Dr. David Ouellet (Pacific Coast Smiles, Santa Maria CA), 100% of patients reviewed showed significant pocket reduction using 1.7% hydrogen peroxide gel and customized application tray. These results demonstrate the efficacy of products like PerioRestore® for patients suffering from periodontal disease, or for prevention and maintenance during and after an orthodontic treatment.
Conclusion
- There is a wide spectrum of quality when it comes to the products and services that clear aligner companies offer, and it can be difficult for consumers to decipher which brands they can entrust with their teeth and wallets.
- When choosing aligners, it is important to choose one that provides gentle but continuous forces and delivers stable forces over time.
- The aligner of choice should be crack- and stain-resistant.
- Choosing an aligner brand that is BPA- and phthalate-free provides a safer aligner for your patients.
- Finish the case with a periodontal home care system to support soft tissue treatment.

Art Kaslow, DDS
Santa Ynez Valley Dental, Solvang, CA

Bora Kilicoglu, PhD, MBA
Global Marketing Manager, DenMa
![]()
Published in TIPS – May/June 2022. Submitted by DenMat.
1. Weir T. Clear Aligners in Orthodontic Treatment. Aus Dent J. 2017;62:58–62. doi: 10.1111/adj.12480. [PubMed] [CrossRef] [Google Scholar]
2. Karkhanechi M, Chow D, Sipkin J, David S, Boylan R, Norman R, et al. Periodontal Status of adult patients treated with fixed buccal appliances and removable aligners over one year of active Orthodontic Theraphy. Angle Orthod. 2013;83:146–51. doi: 10.2319/031212-217.1. [PubMed] [CrossRef] [Google Scholar]
3. Melkos AB. Advances in digital technology and orthodontics: a reference to the Invisalign method. Med Sci Monit. 2005;11:39–42. [PubMed] [Google Scholar]
4. Malik OH, McMullin A, Waring DT. Invisible orthodontics part 1: invisalign. Dent Update. 2013;40:203–4. 207–10, 213–5. doi: 10.12968/denu.2013.40.3.203. [PubMed][CrossRef] [Google Scholar]
5. Graber TM. Orthodontics: Current Principles and Techniques. In: Paquette D, Colville C, Wheeler T, editors. Clear Aligner Treatment. St Louis: Mosby; 2012. pp. 778–811. [Google Scholar]
6. Fujiyama K, Honjo T, Suzuki M, Matsuoka S, Deguchi T. Analysis of pain level in cases treated with Invisalign aligner: comparison with fixed edgewise appliance therapy. Prog Orthod. 2014;15:64. doi: 10.1186/ s40510-014-0064-7. [PMC free article] [PubMed][CrossRef] [Google Scholar]
7. [Accessed October, 2013]. Available from: hhtp://www.invisalign.com/why-invisalign.
8. Miller KB, McGorray SP, Womack R, Quintero JC, Perelmuter M, Gibson J, et al. A comparison of treatment impacts between Invisalign aligner and fixed appliance therapy during the first week of treatment. Am J Orthod Dentofacial Orthop. 2007;131:302.e1–9. doi: 10.1016/j.ajodo.2006.05.031. [PubMed] [CrossRef] [Google Scholar]
9. Proffit WR, Fields H, Sarver D. Contemporary Orthodontics. 5th ed. St. Louis: Mosby; 2013. pp. 355–7. [Google Scholar]
10. Drake C, McGorray S, Dolce C, Nair M, Wheeler T. Orthodontic Tooth Movement with Clear Aligners. ISRN Dent. 2012 doi: 10.5402/2012/657973. doi: 10.5402/2012/657973. [PMC free article] [PubMed][CrossRef] [CrossRef] [Google Scholar]
11. Ponitz RJ. Invisible retainers. Am J Orthod. 1971;59:266–72. doi: 10.1016/0002-9416(71)90099-6. [PubMed] [CrossRef] [Google Scholar]
12. Nahoum H. Forces and moments generated by removable thermoplastic aligners. Am J Orthod Dentofacial Orthop. 2014;146:545–6. doi: 10.1016/j.ajodo.2014.08.006. [PubMed] [CrossRef] [Google Scholar]
13. Barone S, Paoli A, Razionale AV, Savignano R. Computational design and engineering of polymeric orthodontic aligners. Int J Numer Method Biomed Eng. 2017;33 doi: 10.1002/cnm.2839. doi: 10.1002/
cnm.2839. [PubMed] [CrossRef] [CrossRef] [Google Scholar]
14. Kim T, Öztürk Ortan Y. Clear Aligner Appliances: Fabrication and Clinical Application. Turk J Orthod. 2009;22:256–66. doi: 10.13076/1300-3550-22-3-256. [CrossRef] [Google Scholar]
15. Available from: www.ca-clear-aligner.com/en/b2c/index.html
16. Gu J, Tang J, Skulsi B, Fields H, Beck F, Firestone A, et al. Evaluation of Invisalign treatment effectiveness and efficiency compared with conventional fixed appliances using the Peer Assessment Rating index. Am J Orthod Dentofacial Orthop. 2017;151:259–66. doi: 10.1016/j.ajodo.2016.06.041. [PubMed] [CrossRef] [Google Scholar]
17. Wong B. Invisalign A to Z. Am J Orthod Dentofacial Orthop. 2002;121:540–1. doi: 10.1067/mod.2002.123036. [PubMed] [CrossRef] [Google Scholar]
18. Simon M, Keilig L, Schwarze J, Jung B, Bourauel C. Treatment outcome and efficacy of an aligner technique-regarding incisor torque, premolar derotation and molar distalisation. BMC Oral Health. 2014;14:68. doi: 10.1186/1472-6831-14-68. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
19. Lagravère MO, Flores-Mir C. The treatment effects of Invisalign orthodontic aligners: a systematic review. J Am Dent Assoc. 2005;136:1724–9. doi: 10.14219/jada. archive.2005.0117. [PubMed] [CrossRef] [Google Scholar]
20. Kravitz N, Kusnoto B, BeGole E, Obrez A, Agran B. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am J Orthod Dentofacial Orthop. 2009;135:27–35. doi: 10.1016/j.ajodo.2007.05.018. [PubMed] [CrossRef] [Google Scholar]
21. Boissere W, Morton J, Ojima K. Aligner Orthodontics: Diagnostics, Biomechanics Planning and Treatment. Hanover: Quintescence Publishing; 2015. pp. 26–30. [Google Scholar]
22. Sheridan JJ, McMinn R, LeDoux W. Essix thermosealed appliances: various orthodontic uses. J Clin Orthod. 1995;29:108–13. [PubMed] [Google Scholar]
23. Ali SA, Miethke HR. Invisalign, an innovative invisible orthodontic appliance to correct malocclusions: advantages and limitations. Dent Update. 2012;39:254–6. 258–60. doi: 10.12968/denu.2012.39.4.254. [PubMed] [CrossRef] [Google Scholar]
24. Wheeler T. Orthodontic clear Aligner Treatment. Semin Orthod. 2017;23:83–9. doi: 10.1053/j.sodo.2016.10.009. [CrossRef] [Google Scholar]
25. Hennessy J, Al-Awadhi EA. Clear aligners generations and orthodontic tooth movement. J Orthod. 2016;43:68–76. doi: 10.1179/1465313315Y.0000000004. [PubMed][CrossRef] [Google Scholar]
26. Boyd RL. Periodontal and restorative considerations with clear aligner treatment to establish a more favorable restorative environment. Compend Contin Educ Dent. 2009;30:280–2. 284, 286–8. [PubMed] [Google Scholar]
27. Chan E, Darendeliler M. The Invisalign appliance today: A thinking persons orthodontic appliance. Semin Orthod. 2017;23:12–64. doi: 10.1053/j.sodo.2016.10.003. [CrossRef] [Google Scholar]
28. Turley PK. Evolution of esthetic considerations in orthodontics. Am J Orthod Dentofacial Orthop. 2015;148:374–9. doi: 10.1016/j.ajodo.2015.06.010. [PubMed][CrossRef] [Google Scholar]
29. Hennesy J, Garvey T, Al-Awadhi E. A randomized clinical trial comparing mandibular incisor proclination produced by fixed labial appliances and clear aligners. Angle Orthod. 2016;86:706–12. doi: 10.2319/101415-686.1. [PubMed] [CrossRef] [Google Scholar]
30. Kunchio D, Maganzini A, Shelton C, Freeman K. Invisalign and traditional orthodontic treatment post-retention outcomes compared using the American Board of Orthodontics objective grading system. Angle Orthod. 2007;77:864–9. doi: 10.2319/100106-398.1. [PubMed] [CrossRef] [Google Scholar]
31. Djeu G, Shelton C, Maganzini A. Outcome assessment of invisalign and traditional orthodontic treatment compared with the American board of orthodontics objective grading system. Am J Orthod. Dentofacial Orhop. 2005;128:292–8. doi: 10.1016/j. ajodo.2005.06.002. [PubMed] [CrossRef] [Google Scholar]
32. Kassas W, Al-Jewair T, Preston B, Tabba S. Assessment of Invisalign treatment outcomes using the ABO model grading system. J World Fed Orthod. 2013;2:61–4. doi: 10.1016/j.ejwf.2013.03.003. [CrossRef] [Google Scholar]
33. Weihong L, Wang S, Zhang Y. The effectiveness of Invisalign Appliance in extraction cases using the ABO model grading system: a multicenter randomized clinical trial. Int J Clin Exp Med. 2015;8:8276–82. [PMC free article] [PubMed] [Google Scholar] Retracted
34. Hönn M, Göz G. A Premolar Extraction case using the Invisalign System. J Orofac Orthop. 2006;67:385–94. doi: 10.1007/s00056-006-0609-6. [PubMed] [CrossRef] [Google Scholar]
35. Rossini G, Parrini S, Castroflorio T, Deregibus A, Debernardi C. Efficacy of Clear Aligners in controlling Orthodontic Tooth Movement. Angle Orthod. 2015;85:881–9. doi: 10.2319/061614-436.1. [PubMed] [CrossRef] [Google Scholar]
36. Yıldırım A. Doctoral Dissertation. Istanbul University Institute of Health Sciences Orthodontics Department; 2013. A prospective Study to determine the efficiency of Clear Aligner Appliance. [Google Scholar]
37. Skidmore KJ, Brook KJ, Thomson WM, Harding W. Factors influencing treatment time in orthodontic patients 2006. Am J Orthod Dentofacial Orhop. 2006;129:230–8. doi: 10.1016/j.ajodo.2005.10.003. [PubMed] [CrossRef] [Google Scholar]
38. Buschang PH, Shaw SG, Ross M, Crosby D, Campbell PM. Comparative time efficiency of aligner therapy and conventional edgewise braces. Angle Orthod. 2014;84:391–6. doi: 10.2319/062113-466 [PubMed] [CrossRef] [Google Scholar]
39. Bradley TG. Changes in orthodontic treatment modalities in the past 20 years: exploring the link between technology and scientific evidence. J Ir Dent Assoc. 2013;59:91– 4. [PubMed] [Google Scholar]
40. Han JY. A comparative study of combined periodontal and orthodontic treatment with fixed appliances and clear aligners in patients with periodontitis. J Periodontal Implant Sci. 2015;45:193–204. doi: 10.5051/jpis.2015.45.6.193. [PMC free article] [PubMed][CrossRef] [Google Scholar]
41. Levrini L, Mangano A, Montanari P, Margherini S, Caprioglio A, Abbate GM. Periodontal health status in patients treated with the Invisalign (®) system and fixed orthodontic appliances: A 3 months clinical and microbiological evaluation. Eur J Dent. 2015;9:404–10. doi: 10.4103/1305-7456.163218. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
42. Abbate GM, Caria MP, Montanari P, Mannu C, Orrù G, Caprioglio A, et al. Periodontal health in teenagers treated with removable aligners and fixed orthodontic appliances. J Orofac Orthop. 2015;76:240–50. doi: 10.1007/s00056-015-0285-5. [PubMed] [CrossRef] [Google Scholar]
43. Türkkahraman H, Sayin MO, Bozkurt FY, Yetkin Z, Kaya S, Onal S. Archwire ligation techniques, microbial colonization, and peri- odontal status in orthodontically treated patients. Angle Orthod. 2005;75:231–6. [PubMed] [Google Scholar]
44. Azeem M, Ul Hamid W. Incidence of White Spot lesions during Clear Aligner Theraphy. J World Fed Orthod. 2017;6:127–30. doi: 10.1016/j.ejwf.2017.07.001. [CrossRef] [Google Scholar]
45. Tieu LD, Saltaji H, Normando D, Flores-Mir C. Radiologically determined orthodontically induced external apical root resorption in incisors after non-surgical orthodontic treatment of class II division 1 malocclusion: a systematic review. Prog Orthod. 2014;15:48. doi: 10.1186/s40510-014 0048-7. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
46. Iglesias-Linares A, Sonnenberg B, Solano B, Yañez-Vico RM, Solano E, Lindauer SJ, et al. Orthodontically induced external apical root resorption in patients treated with fixed appliances vs removable aligners. Angle Orthod. 2017;87:3–10. doi: 10.2319/02016-101.1. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
47. Linge L, Linge BO. Patient characteristics and treatment variables associated with apical root resorption during orthodontic treatment. Am J Orthod Dentofacial Orthop. 1991;99:35–43. doi: 10.1016/S0889-5406(05)81678-6. [PubMed] [CrossRef] [Google Scholar]
48. Roscoe MG, Meira JB, Cattaneo PM. Association of orthodontic force system and root resorption: A systematic review. Am J Orthod Dentofacial Orthop. 2015;147:610–26. doi: 10.1016/jajodo.2014.12.026. [PubMed] [CrossRef] [Google Scholar]
49. Gay G, Ravera S, Castroflorio T, Garino F, Rossini G, Parini S, et al. Root resorption during orthodontic treatment with Invisalign: a radiometric stu
50. Zheng M, Liu R, Ni Z, Yu Z. Efficiency, effectiveness and treatment stability of clear aligners: A systematic review and meta-analysis. Orthod Craniofac Res. 2017;20:127–133. doi: 10.1111/ocr.12177. [PubMed] [CrossRef] [Google Scholar]
Category: Merchandise
Back to Articles